General medicine case 20-06-22
Welcome and greetings to every one who are visiting my blog. This is A.Sai Tarun of 5th semester. This is an online E log platform to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. I have been given this case in order to solve in an attempt to understand the topic of patient's clinical data analysis to develop my competency in reading and comprehending clinical data and come up with a diagnosis and treatment plan.
DATE OF ADMISSION - 19/06/22
Introduction
-55 yr old female Patient came to OPD with chief complaints of fever,chills,vomitings and burning sensation of both feet
HISTORY OF PAST ILLNESS
PERSONAL HISTORY
•Mixed diet
Appetite Normal
•Sleep adequate
•Bowel and Bladder movements regular.
TREATMENT HISTORY
FAMILY HISTORY
• Not significant.
•S1, S2 heard
•No murmurs
RESPIRATORY SYSTEM:
•NVBS heard
•Position of trachea - central
•Breath sounds - vesicular
ABDOMEN
•Shape - obese
•No Tenderness
•No palpable mass
•No free fluid
•Spleen and liver not palpable
CENTRAL NERVOUS SYSTEM:
•Intact
•No focal defect
•No abnormality detected
CEREBRAL SIGNS
• No finger nose incordination
•No knee heel incordination.
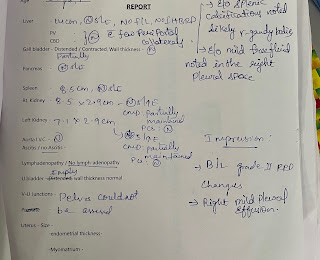
INVESTIGATIONS
























Comments
Post a Comment